|
News Detail
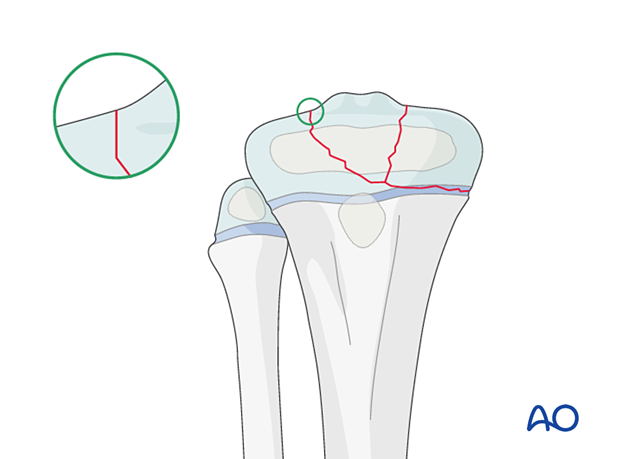
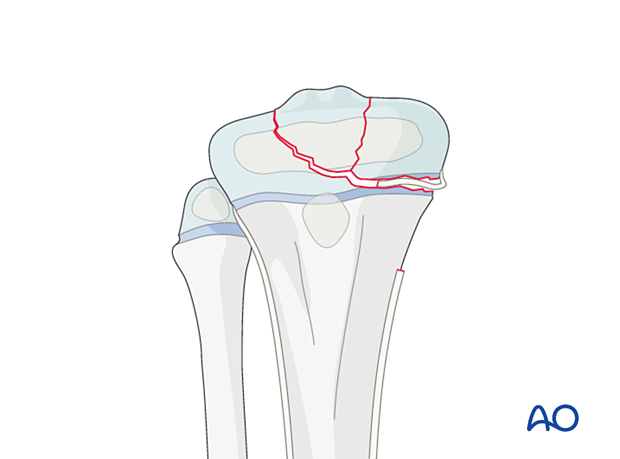
Open reduction - Plate fixation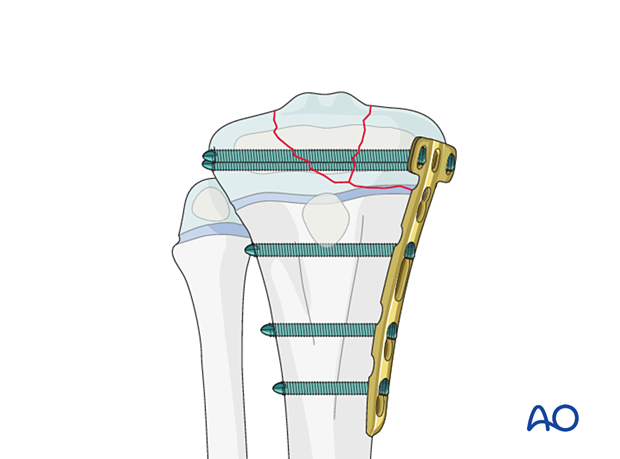 1. General considerations Introduction Multifragmentary Salter-Harris III and IV fractures require open reduction and plate fixation, spanning the physis. The plate position is dictated by the configuration of the fracture. The use of locking head screws avoids compression of the perichondral ring. The epiphyseal screws must be removed as soon as bone healing allows to prevent growth arrest and deformity.
It is mandatory to achieve anatomical reduction of the articular surface to preserve joint function. Open reduction is therefore necessary. The main goals of treatment of these fractures are to: Restore joint congruity Minimize injury to the physis Prevent secondary displacement
Size and type of implant 2.0–4.5 mm plates are typically used in pediatric practice. The age and weight of the patient, the anatomical site, and the load to which they will be subjected dictate the size of the implant. A T-shaped plate can be used. Adult anatomic plates for the proximal tibia can be used in older children.
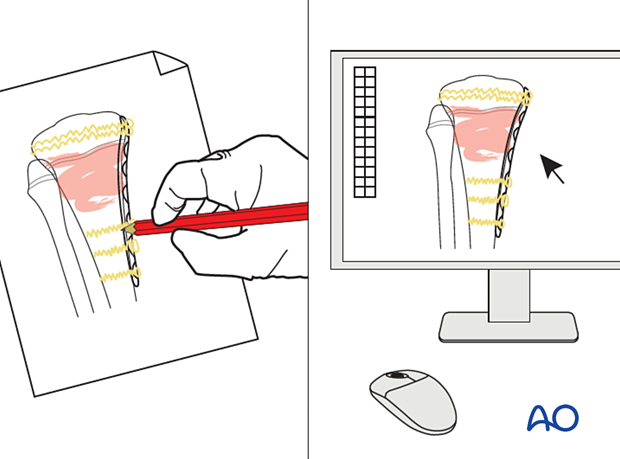
2. Preoperative planning Preoperative planning is an essential part of the treatment of all proximal tibial fractures because of the variability of the fracture pattern and patient characteristics. This involves: Careful study of the x-rays Definition of the fracture fragments and the desired result. This may be achieved with appropriate software Choice of implants
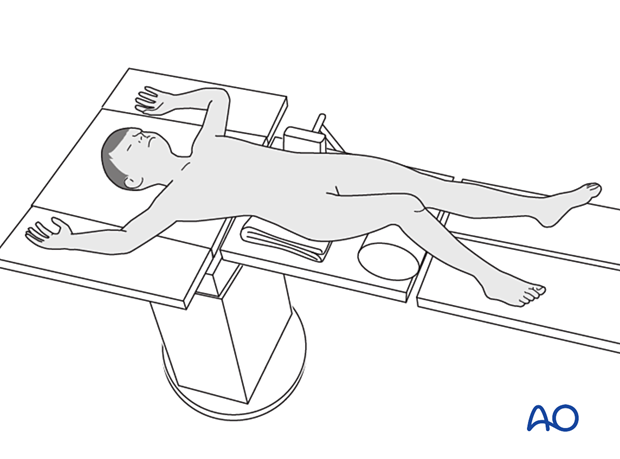
3. Patient preparation Place the patient in a Breaking the table to allow knee flexion may facilitate traction and reduction.
4. Approaches Confirm the location of the physis with an image intensifier and protect the perichondral ring and adjacent periosteum. These fractures are typically managed with an Arthroscopy 5. Reduction Removal of impediments It may be necessary to remove interposed soft tissue and periosteum without devitalizing the fracture fragments. This is performed under direct vision, prior to fracture reduction.
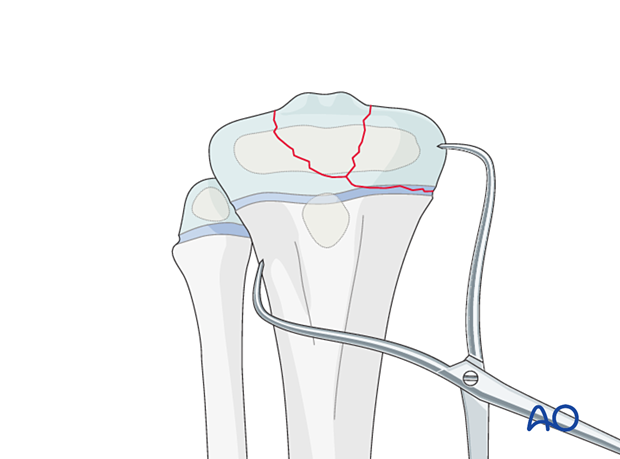
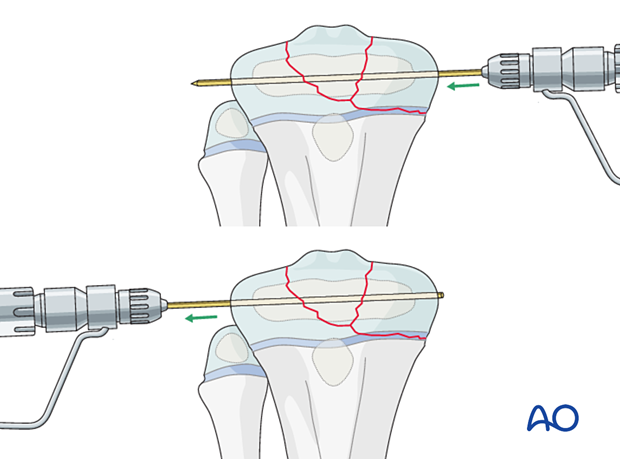
Reduction maneuvers Reduction can be performed with traction and pointed reduction forceps. K-wire joysticks are particularly useful to reduce intraarticular fragments. Confirm anatomical reduction of the articular surface under direct vision and of the physis with an image intensifier.
Temporarily stabilize the fracture with a K-wire. Advance the K-wire through the opposite soft tissues and pull it through until its end is flush with the cortex avoiding interference with the plate. Take care not to damage the common peroneal nerve.
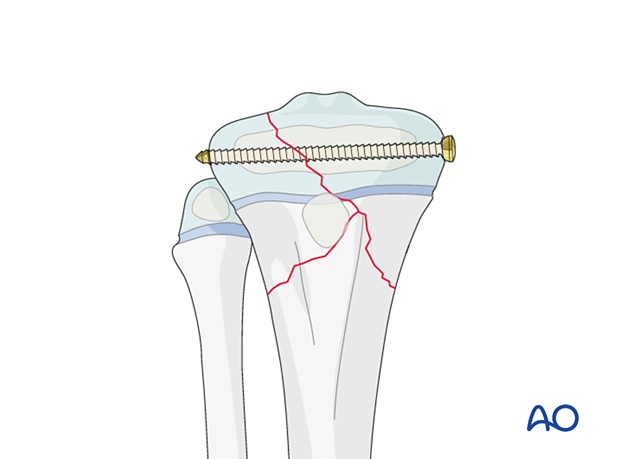
6. Epihyseal screw fixation In some Salter-Harris IV fractures, the epiphysis may be stabilized with an interfragmentary screw prior to plate fixation. This allows for better reduction and fixation of the articular surface. Plan the screw trajectory to avoid conflict with later plate application.
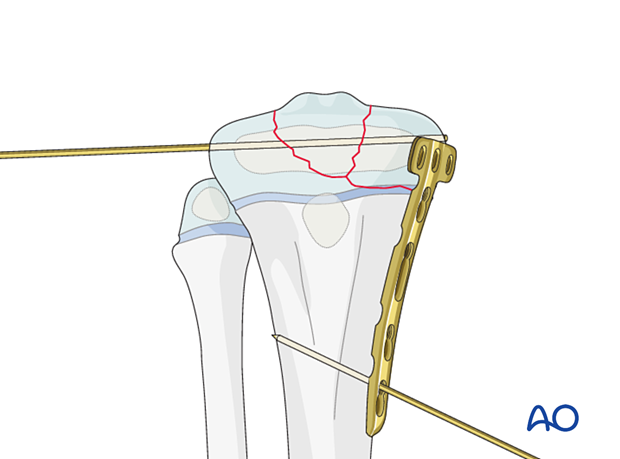
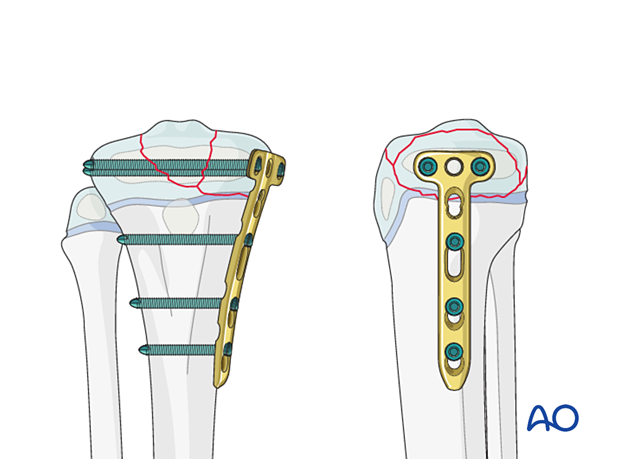
7. Plate fixation Apply the plate without compressing the physis. Plate application Contour the plate to match the anatomy of the proximal tibia. Place the plate so that the proximal screws can be inserted into the epiphysis, parallel to the physis. Hold the plate to the bone with K-wires.
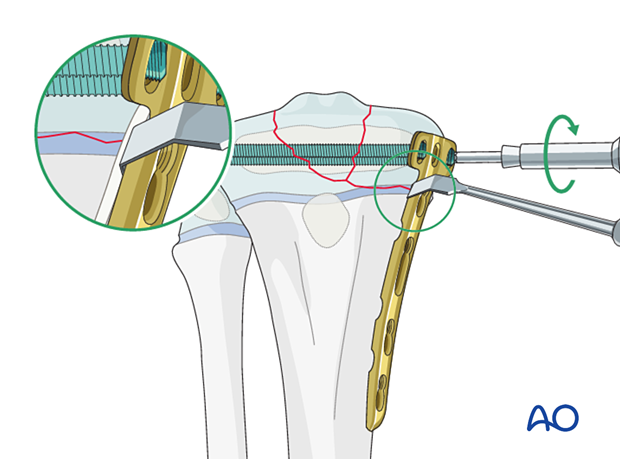
Screw insertion The periosteum and perichondral ring should not be disturbed. Locking screws should be used adjacent to the physis to prevent compression of the perichondral ring. To protect the perichondral ring, a dissector or elevator may be used to offset the plate during locking screw insertion.
Before screw insertion, ensure that both plate ends are aligned and have good contact with the bone. Check the tibial alignment with an image intensifier before screw insertion. The order of screw insertion depends on the fracture configuration. Remove the dissector or elevator after screw fixation. Remove the temporary K-wire.
8. Final assessment Confirm fracture reduction and implant position with an image intensifier. 9. Application of a splint In a patient compliant with weight-bearing restrictions, no additional casting is necessary. A 10. Aftercare Immediate postoperative care The patient is kept touch-weight bearing. Older children may be able to use crutches or a walker. Younger children may require a period of mobilization in a wheelchair. If no cast has been applied, range of motion exercises can be started immediately.
Neurovascular examination The patient should be examined frequently in the initial period following the injury, to exclude neurovascular compromise or evolving compartment syndrome. High-energy fractures are associated with vascular injuries and require careful clinical assessment. Follow-up The first clinical and radiological follow-up is usually undertaken at 4–6 weeks. Mobilization Weight bearing can be started when clinical and radiological signs suggest a stable fracture, typically 3–4 weeks after injury. Implant removal Early implant removal should be performed after clinical and radiographic confirmation of fracture consolidation to avoid growth arrest. Alternatively, if there is remaining growth, the epiphyseal screws should be removed after initial fracture healing. The remaining implant may be removed later if necessary. Follow-up for growth disturbance All patients with fractures of the proximal tibia should have clinical and radiological examination 8–12 weeks postoperatively to confirm healing and alignment. Clinical examination should be repeated at intervals for at least one year to detect early signs of growth disturbance. If there is a clinically relevant leg length discrepancy or malalignment, radiological assessment is required.
|

Shanghai Carefix Medical Instrument Co., Ltd.China
滬ICP備16042301號-1 (滬)-非經(jīng)營性-2016-0122 滬食藥監(jiān)械生產(chǎn)許20101725號
