|
News Detail
AO Surgery Reference:Distal femoral fracture (Hoffa fracture) - internal fixation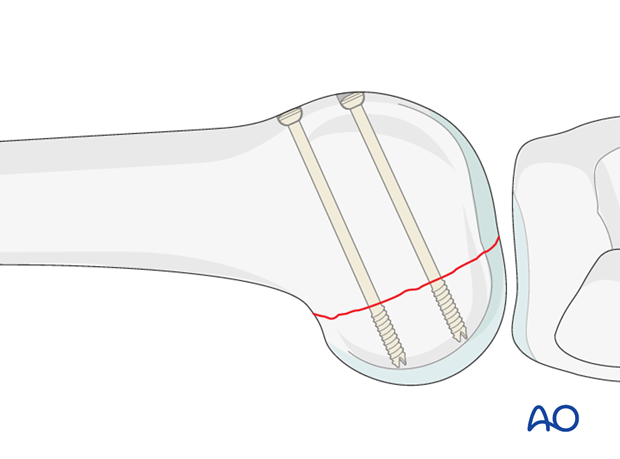
ORIF - Anterior lag screws for large fragments33B3.2/.3 Partial articular fracture, frontal/coronal, posterior condyle(s)5/5 – Aftercare
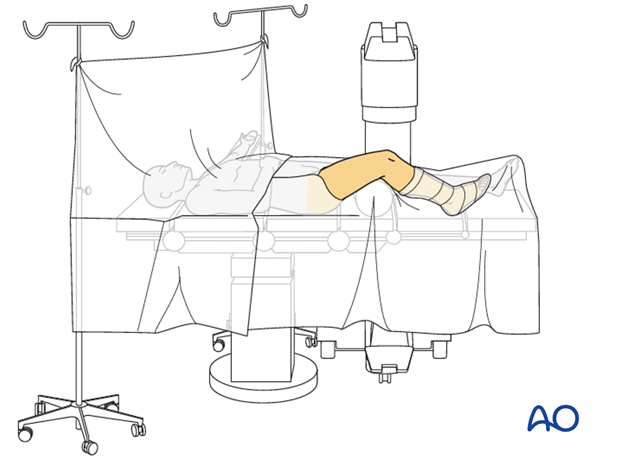
1. PrinciplesHoffa fractures involve important load-bearing areas of the knee joint surface, and the principles of anatomical reduction and absolute stability of fixation apply. Generally, these fractures are reduced and fixed from posterior with leg screws and a buttress plate. However, occasional circumstance would only allow for anterior fixation alone. This fixation is not stable and is generally not advised. Fixation from anterior can be achieved indirectly with 3.5 mm or 4.5 mm screw systems. It is advantageous to use cannulated screw systems. In small fragments direct fixation through a posterior approach is required. At least two screws should be used, in order to prevent fragment rotation and to achieve satisfactory compression. No implant can violate the articular surface. Similar principles apply if both condyles are fractured. 2. Preparation and approachPositioningThis procedure may be performed with the patient in one of the following positions:
 ApproachFor this procedure the following approaches may be used:
These difficult fractures can be approached for reduction and fixation from the anterior aspect. If the posterior condylar fragments are large, the fracture lines will usually be accessible by the parapatellar approach. For shallower fragments the standard lateral/anterolateral approach is necessary to gain more posterior access: alternatively, a posterior approach should be considered. For the medial side, a straight medial approach can be used, taking care to avoid injury to the infrapatellar branch of the saphenous nerve. 3. ReductionAchieve reduction using periosteal elevators and a large pointed reduction forceps. The joystick technique, in which a small Schanz screw is inserted from the extraarticular surface, is also useful (as illustrated). 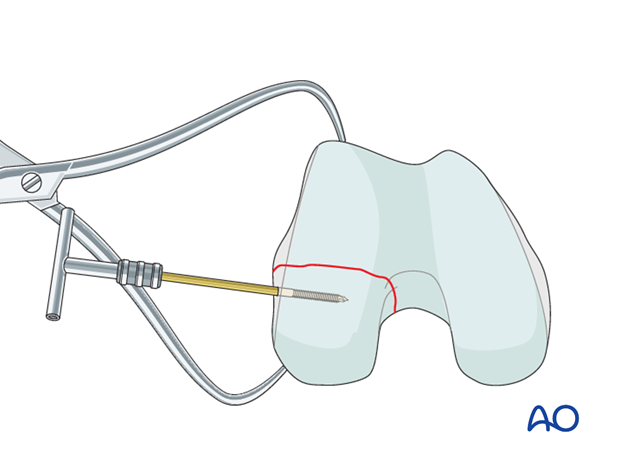 4. FixationGuide-wire insertionInsert the guide wires as perpendicularly as possible to the fracture plane. 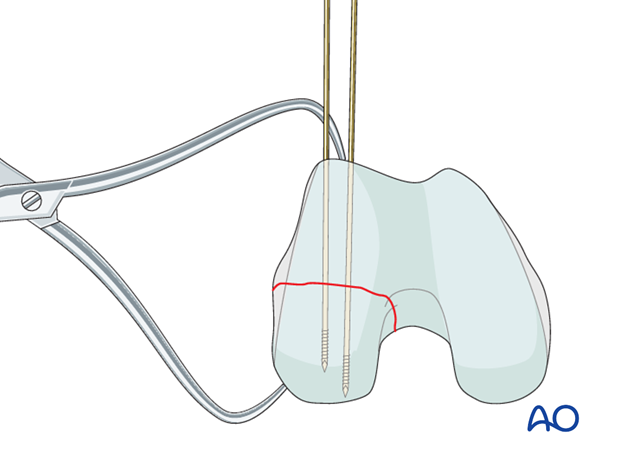 Check guide-wire placementCheck the correct guide-wire insertion under fluoroscopic image intensifier control. The condylar surface must not be perforated. 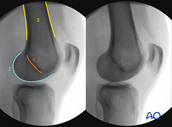 Optimal views and anatomical landmarksIntraoperative imaging of the knee 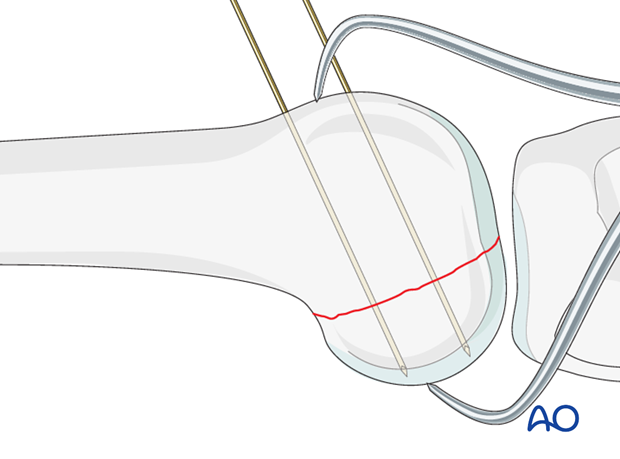 Screw insertionThe lag screws are inserted according to the standard technique for cancellous lag screws under image intensifier control.
There should be no protruding screw heads. X-rayX-ray showing the completed osteosynthesis. In this instance this fixation has worked over long term. Generally, a posterior buttress plate should also be used. 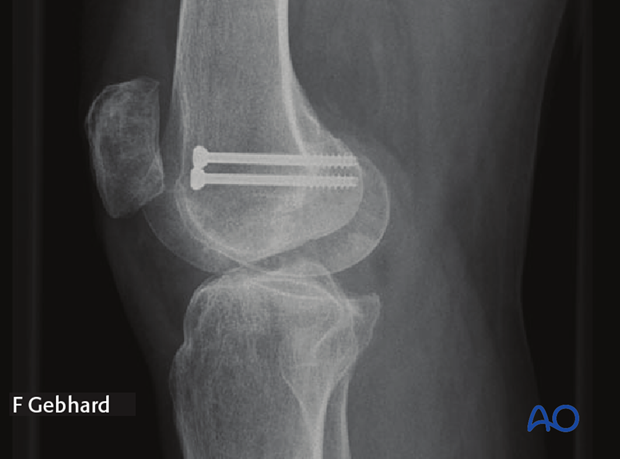 5. AftercareImpediments to the restoration of full knee function after distal femoral fracture are fibrosis and adhesion of injured soft tissues around the metaphyseal fracture zone, joint capsular scarring, intra-articular adhesions, and muscle weakness. Early range of motion helps restore movement in the early postoperative phase. With stable fracture fixation, the surgeon and the physical therapy staff will design an individual program of progressive rehabilitation for each patient. The regimens suggested here are for guidance only and not to be regarded as prescriptive. Functional treatmentUnless there are other injuries or complications, knee mobilization may be started immediately postoperatively. Both active and passive motion of the knee and hip can be initiated immediately postoperatively. Emphasis should be placed on progressive quadriceps strengthening and straight leg raises. Static cycling without load, as well as firm passive range of motion exercises of the knee, allow the patient to regain optimal range of motion. 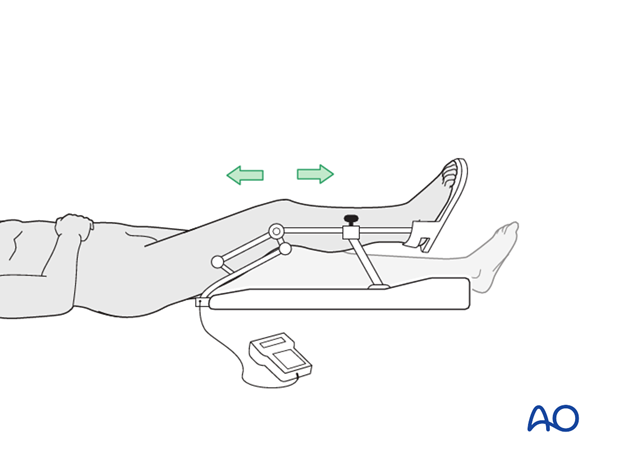 Weight bearingTouch-down weight-bearing (10-15 kg) may be performed immediately with crutches, or a walker. This will be continued for 6-10 weeks postoperatively. This is mostly to protect the articular component of the injury, rather than the shaft injury. Touch-down weight-bearing progresses to full weight-bearing gradually, over a period of 2 to 3 weeks (beginning at 6–10 weeks postoperatively). Ideally, patients are fully weight-bearing, without devices (e.g., cane) by 12 weeks. Follow-upWound healing should be assessed at two to three weeks postoperatively. Subsequently 6-week, 12-week, 6-month, and 12-month follow-ups are usually made. Serial x-rays allow the surgeon to assess the healing of the fracture. Implant removalImplant removal is not essential but should be discussed with the patient if there are implant-related symptoms after consolidated fracture healing. Thrombo-embolic prophylaxisThrombo-prophylaxis should be given according to local treatment guidelines. ORIF - Lag screw from posterior with or without plate33B3.2/.3 Partial articular fracture, frontal/coronal, posterior condyle(s)6/6 – Aftercare
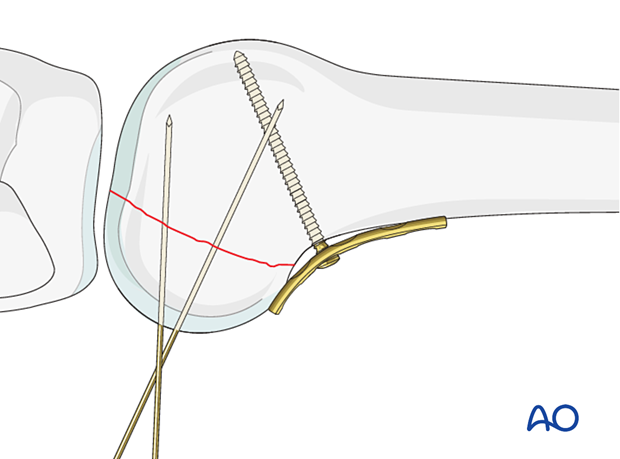
1. PrinciplesGeneral considerationsHoffa fractures involve important load-bearing areas of the knee joint surface, and the principles of anatomical reduction and absolute stability of fixation apply. In general, a buttress plate with lag screws is recommended. However, if the fragment is small, then isolated lag screws may be the only fixation possible. The indirect lag screw technique from anterior is not recommended as the thread will be too long and will not achieve adequate stability and compression of the fragment. Similar principles apply if both condyles are fractured. 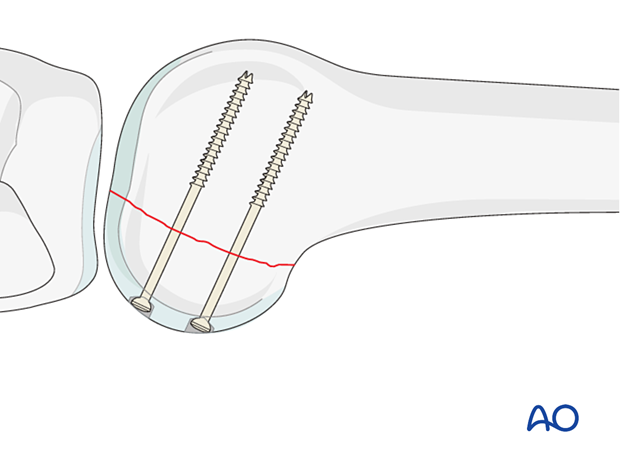 Screw typesNone of the implants can project above the articular surface. This can be achieved by countersunk lag screws (A) or headless compression screws (B). At least two screws should be used, in order to prevent fragment rotation For this procedure, 3.5 mm cannulated headless compression screws or standard 3.5 mm lag screws can be used. However, different size screws can be used depending on fragment size. 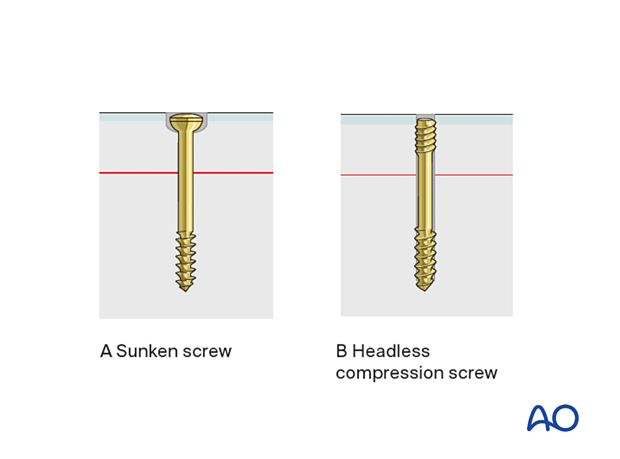 2. Patient preparation and approachPatient preparationThe procedure is performed with the patient placed supine and the knee flexed 20-30°. ApproachFor lateral Hoffa injuries, the Swashbuckler approach or the Gerdytubercle osteotomy approach is used. For medial Hoffa injuries, the internervous medial approach is used. 3. ReductionReduce the fracture using a small ball-spiked pusher and secure it temporarily with a K-wires. Make sure that the K-wires does not conflict with the planned plate position and screw track. 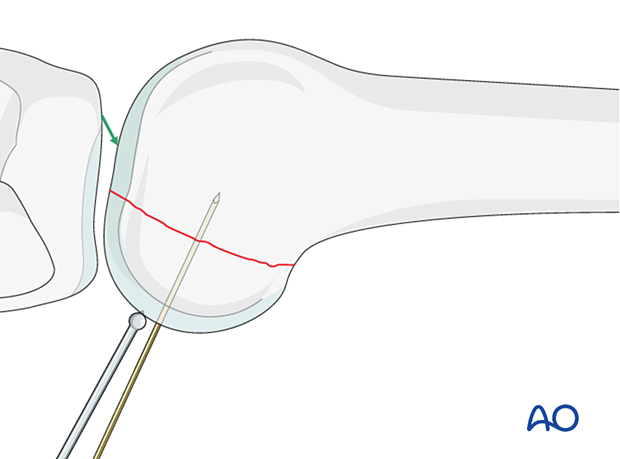 4. FixationPrincipleTo enhance the stability and to avoid axial load on the fracture (especially in the osteoporotic bone), a buttress plate is needed to prevent cranial displacement of the fragment. The plate needs to be placed according to the position of the unstable fracture fragment. Occasionally this fracture fragment is lateral. A wide range of plates can be utilized and as an example, we will here use a simple slightly under-contoured 3.5 mm narrow plate. Plate applicationApply the plate to the posterior aspect of the distal femur. This plate will need to be positioned as far distal as possible without affecting the articular surface. To press the under-contoured plate firmly to the femur, insert a standard cortical screw just proximal to the fracture line in neutral mode.
 Secure the plate with one or more bicortical cortical screws proximal to the first screw. Additional screws can be inserted in the distal aspect of the plate if they fit on the non-articular surface. All these screws are inserted in neutral mode. 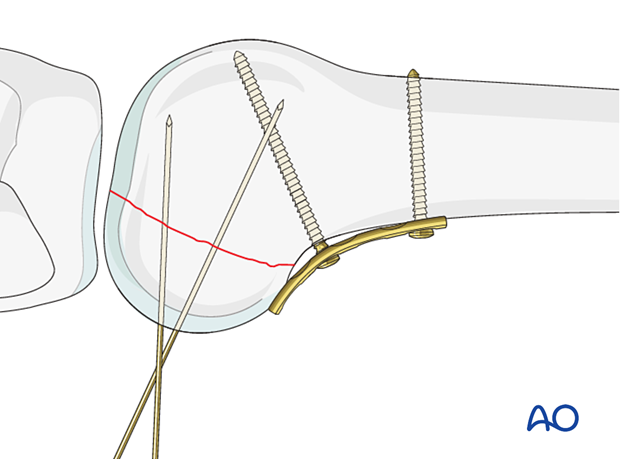 This intraoperative image demonstrates an operation where the posterior Hoffa has been reduced and held temporarily with a K-wire and buttressed with a posterior plate. 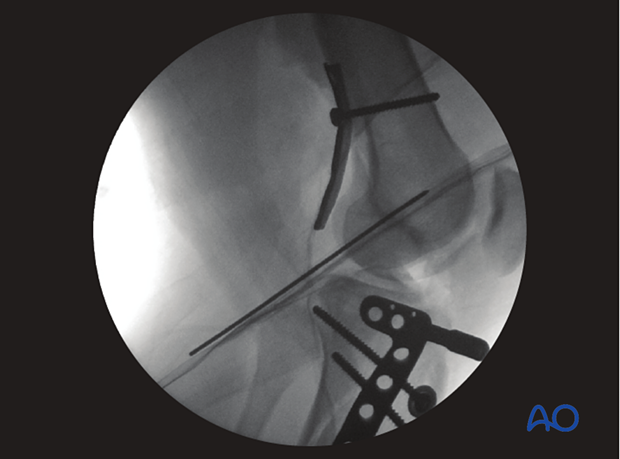 Postoperative image with posterior buttress plate in place. 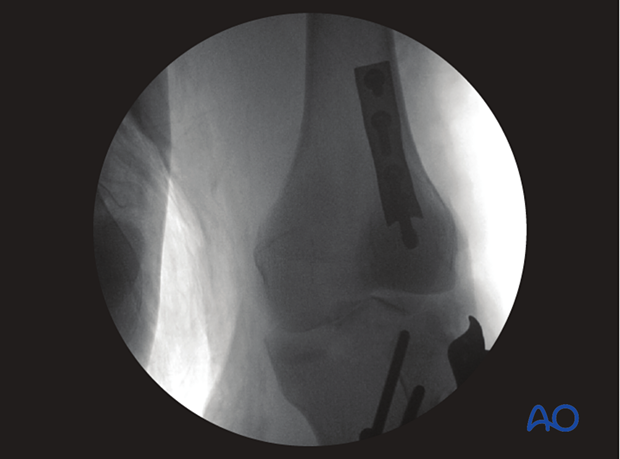 Guide-wire insertionInsert two guide wires perpendicular to the fracture plane. Make sure not to penetrate the far cortex. 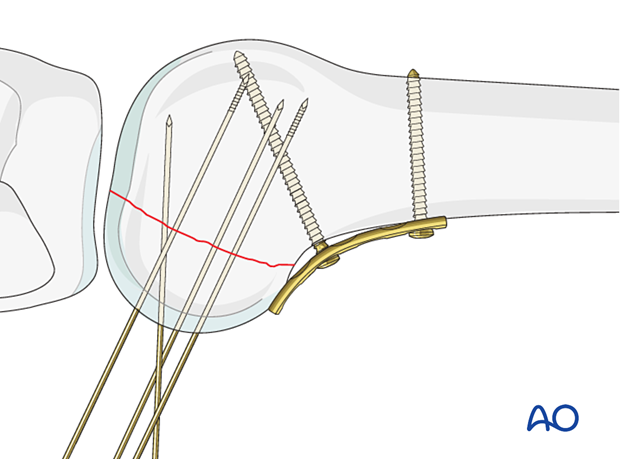 Check guide-wire insertionCheck the guide-wire position under image intensifier control, in the lateral and oblique views. Optimal views and anatomical landmarksIntraoperative imaging of the knee 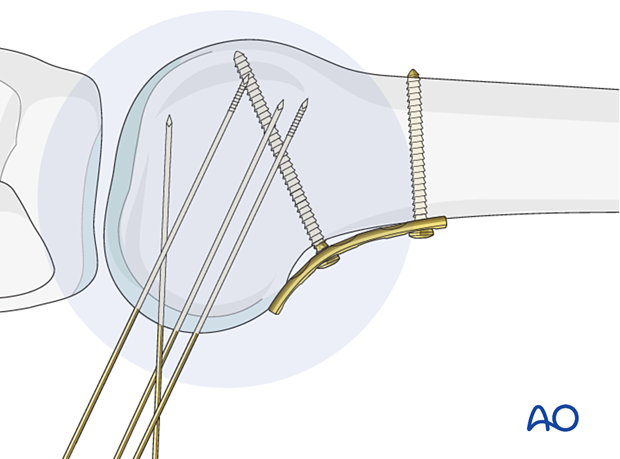 Headless compression screw insertionInsert headless compression screws, using the cannulated screwdriver, and check under image intensifier control in the lateral view that the screw length was chosen appropriately.
 Alternative: Standard screwsThe lag screws are inserted according to the standard technique for cancellous lag screws under image intensifier control. Care is taken to countersink in order to prevent protruding screw heads.  5. CaseFixation failure, as seen here, is common when the plate is placed laterally or medially instead of posteriorly. This image shows articular incongruity which must be operated upon a second time.  6. AftercareImpediments to the restoration of full knee function after distal femoral fracture are fibrosis and adhesion of injured soft tissues around the metaphyseal fracture zone, joint capsular scarring, intra-articular adhesions, and muscle weakness. Early range of motion helps restore movement in the early postoperative phase. With stable fracture fixation, the surgeon and the physical therapy staff will design an individual program of progressive rehabilitation for each patient. The regimens suggested here are for guidance only and not to be regarded as prescriptive. Functional treatmentUnless there are other injuries or complications, knee mobilization may be started immediately postoperatively. Both active and passive motion of the knee and hip can be initiated immediately postoperatively. Emphasis should be placed on progressive quadriceps strengthening and straight leg raises. Static cycling without load, as well as firm passive range of motion exercises of the knee, allow the patient to regain optimal range of motion. Weight bearingTouch-down weight-bearing (10-15 kg) may be performed immediately with crutches, or a walker. This will be continued for 6-10 weeks postoperatively. This is mostly to protect the articular component of the injury, rather than the shaft injury. Touch-down weight-bearing progresses to full weight-bearing gradually, over a period of 2 to 3 weeks (beginning at 6–10 weeks postoperatively). Ideally, patients are fully weight-bearing, without devices (e.g., cane) by 12 weeks. Follow-upWound healing should be assessed at two to three weeks postoperatively. Subsequently 6-week, 12-week, 6-month, and 12-month follow-ups are usually made. Serial x-rays allow the surgeon to assess the healing of the fracture. Implant removalImplant removal is not essential but should be discussed with the patient if there are implant-related symptoms after consolidated fracture healing. Thrombo-embolic prophylaxisThrombo-prophylaxis should be given according to local treatment guidelines.
|

Shanghai Carefix Medical Instrument Co., Ltd.China
滬ICP備16042301號-1 (滬)-非經(jīng)營性-2016-0122 滬食藥監(jiān)械生產(chǎn)許20101725號
