療器械有限公司")
|
News Detail
External fixator device care for an infant, child and young person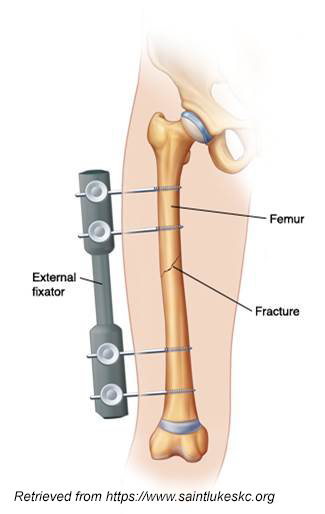 Introduction
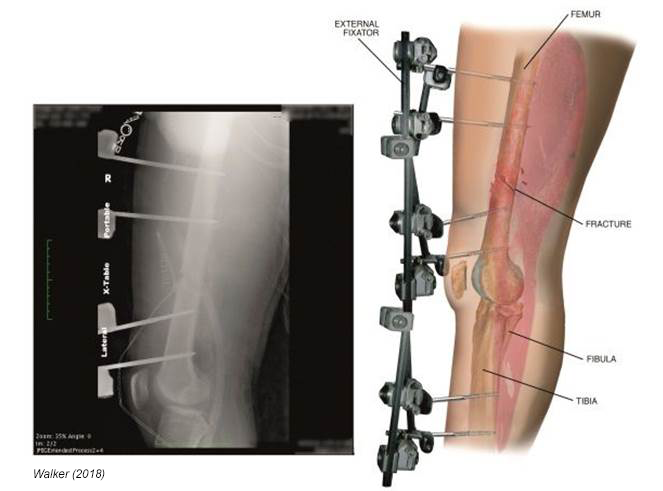
An external fixator is an orthopaedic device wherein an external frame is affixed to the skeleton through pins to facilitate healing, in the case of fracture management, or limb lengthening to manage growth abnormalities. Framed ex-fixes are usually made up of rings made from stainless steel or carbon-fiber. Pins attached to the frame then pass through the skin, soft tissue and into the bone. Simple ex-fix devices typically consist on the external linear frame or strut, with pins attaching to the bone. Rods may be used to adjust the frames or length once they’re in place. External fixators used at Starship Child Health: Ilizarov frames Taylor Spatial frames (picture left) Simple Ex-fix- Usually named for the limb it is applied to (pictured right) External fixators in practice The rationale for external fixators may be to manage complex fracture or fractures which have failed to unionize satisfactorily. Non-union or mal-union may occur due to infection or other complications, using traditional fixation such as internal metal-ware and therefore require further reconstruction. In this context the application of an external fixator is to maintain the corrected position. Alternatively, an ex-fix such as a Taylor Spatial frame may be applied to facilitate bone growth to correct bone length abnormalities. Nursing considerations External fixators in practice contribute to significant disruption of both lifestyle and comfort. Activities of daily living such as bathing and toileting with an external fixator may create new areas of dependency for previously independent patients. This can be particularly challenging for adolescent patients. Nursing care should include early referral to allied health as well as initiating conversations around strategies for managing daily tasks, and recognising the impact these disruptions may have on the patients mental health and body image.
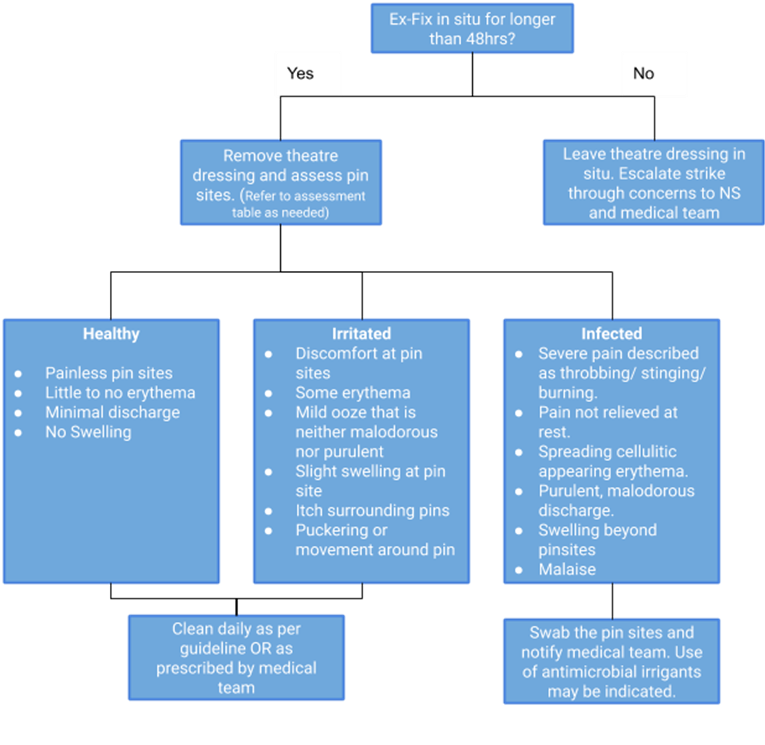
Ongoing difficulty in coping with the external fixator can be associated with poor care compliance and therefore higher rates of complication. Concerns around a patient’s coping with the frame should be promptly escalated to their nurse specialist or registrar. Initiating early education on pin site assessment and care empowers patients and their whānau to have confidence to care for their child on discharge. Neurovascular monitoring Care in the immediate post-operative period Leave the theatre dressing in place for at least the first 48 hours post operatively unless explicitly documented in the post-operative plan. This encourages pin site healing, and reduces infection risk. If dressings are noted to have significant ooze or strike-through within the initial period, this requires escalation to the responsible Orthopaedic team and the patient’s nurse specialist. Potential complications Pin site infection Frame or pin failure/loosening Skin migration up pin Osteomyelitis Mal-union Non-union Neurovascular injury Compartment syndrome Re-fracture around pin Care of pin sites
Pin site infection is recognised among the most common complications of external fixation application. Pin site cares, following the initial 48-hour period, serves to significantly minimise infection risk, prevents tenting at the pin site and provides an opportunity for pin sites to be inspected for early signs of infection. Targeted daily pin site cleaning refers to intentional cleaning and care of pin sites with irrigation solution and gauze or cotton buds. Targeted cleaning can be replaced by showering with hot soapy water when pin sites are clean and free of erythema and tracking. When the pin sites are able to be cleaned as part of an ordinary shower targeted pin site cares are only required weekly. When pin sites appear erythematous or are producing new ooze, the frequency of cares should be directed by the orthopaedic team. The goal of pin site cares are: Daily thorough pin site inspection Removal of irritants to surrounding skin, and skin protection Prevent tenting or migration of skin at pin sites Irrigation solutions The use of normal saline is recommended for non-infected, daily pin site cleaning. Alternative solutions may be used only as directed and prescribed by the orthopaedic team. Alternative solutions may cause local skin irritation and be uncomfortable for the child. Infection or suspected infection may warrant the use of anti-microbial solutions such as chlorhexidine only as directed by the orthopaedic team. Infected pin sites require bacterial wound swabs, photographs and occasionally further pharmacological management. Pin site cleaning technique
Pin site cleaning is done with cotton buds and the appropriate irrigation solution. Sterile cotton bud packs are opened part way to create a pocket, the irrigation solution is poured into the pocket so that the solution covers the whole cotton tip. Each pin site is cleaned with a different cotton bud. It is important that each cotton bud or piece of gauze is only used on one pin site. The cotton bud is pressed firmly against the exit site of the pin and tracked circumferentially around the pin, clearing any ooze that adheres to the pin site. Ensure the granulation tissue is left in place as this encourages healing of the sites and reduces the risk of pin site infection. Dressings Pressure dressings may be required over pins where the surrounding skin is under significant tension, is tenting up the pin or has been found to migrate creating tracking at the pin sites. Simple Mepitel and gauze dressings can serve to reduce skin puckering and hyper-granulation at the pin site. Silver impregnated dressings may be advantageous as management or prophylaxis for pin site infection. A dressing can be fitted to the pin sites by cutting a channel in the dressing and fitting it around the pin as pictured above. Pain management Some patients may find pin site cares distressing and painful initially. Regular basic analgesia should be administered prior to the pin site cares in the acute phase however pain is expected to improve over time. Distraction therapy is particularly beneficial for preparation of the child prior to and during pin site cares to promote a more positive experience leading up to discharge. Nitrous oxide or other forms of pain management may be required initially as perprocedural pain management guideline.
|



Shanghai Carefix Medical Instrument Co., Ltd.China
滬ICP備16042301號(hào)-1 (滬)-非經(jīng)營(yíng)性-2016-0122 滬食藥監(jiān)械生產(chǎn)許20101725號(hào)
