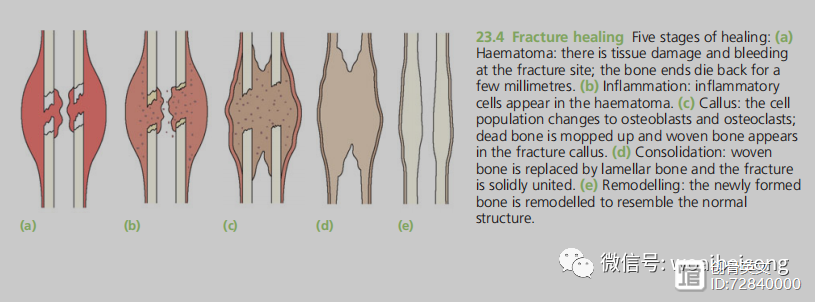
HEALING BY CALLUS
This is the 'natural’ form of healing in
tubular bones; in the absence of
rigid fixation,
it proceeds in five stages:
1.
Tissue destruction and
haematoma
formation
–
Vessels are torn
and a haematoma forms around and within the fracture. Bone at the fracture surfaces,
deprived
of a blood supply, dies back for a
millimetre
or two.
2.
Inflammation and cellular proliferation
– Within 8 hours of the fracture there is an
acute inflammatory reaction
with
migration
of inflammatory cells and the initiation of
proliferation
and
differentiation of mesenchymal stem cells
from the periosteum, the
breached medullary canal
and the surrounding muscle. The fragment ends are surrounded by cellular tissue, which creates a
scaffold
across the fracture site.
A vast array of inflammatory mediators (cytokines and various growth factors) is involved.
The clotted haematoma is slowly absorbed and fine new capillaries grow into the area.
3.
Callus formation
– The differentiating stem cells provide
chrondrogenic
and
osteogenic cell
populations; given the right conditions – and this is usually the local biological and
biomechanical
environment – they will start forming bone and, in some cases, also
cartilage. The cell population now also includes
osteoclasts
(probably
derived from
the new blood vessels), which begin to
mop up
dead bone. The thick cellular mass, with its islands of
immature
bone and cartilage, forms the
callus or splint
on the
periosteal and endosteal surfaces.
As the immature fibre bone (or 'woven’ bone) becomes more
densely mineralized, movement at the fracture site decreases progressively and at about 4 weeks after injury the fracture 'unites’.
4.
Consolidation
– With continuing osteoclastic and osteoblastic activity the woven bone
is transformed intolamellar bone. The system is now rigid enough to allow osteoclasts to
burrow
through the debris at the fracture line, and close behind them.
Osteoblasts
fill in the remaining gaps between the fragments with new bone. This is a slow process and it may be several months before the bone is strong enough to carry normal loads.
5.
Remodelling
– The fracture has been bridged by
a cuff of
solid bone. Over a period of months, or even years, this crude 'weld’ is reshaped by a continuous process of
alternating bone resorption and formation.
Thicker lamellae are laid down where the stresses are high, unwanted buttresses are carved away and the medullary cavity is reformed.
Eventually, and especially in children, the bone
reassumes
something like its normal shape.
---from
《Apley’s System of Orthopaedics and Fractures》P690
療器械有限公司")

