|
News Detail
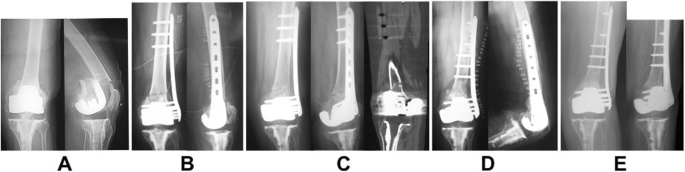
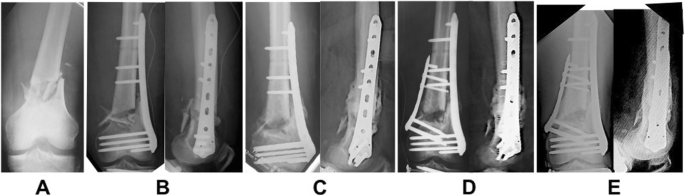
Clinical outcomes of treatment with locking compression plates for distal femoral fractures in a ret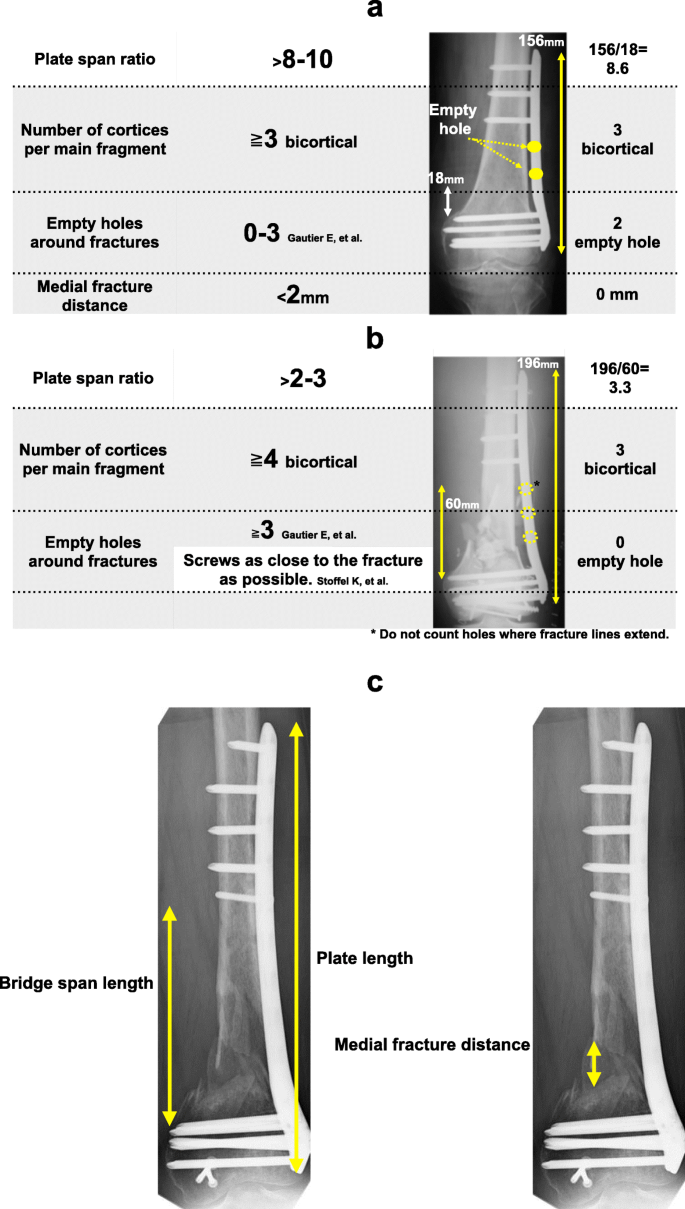 Abstract Background Plate fixation is one of the standard surgical treatments for distal femoral fractures. There are few reports on the relationship between the screw position and bone union when fixing by the bridging plate (relative stability) method. Methods This retrospective study included 71 distal femoral fractures of 70 patients who were treated with the locking compression plate for distal femur (DePuy Synthes Co., Ltd, New Brunswick, CA, USA). The following measurements were evaluated and analyzed: (1) bone union rate, (2) bridge span length (distance between screws across the fracture), (3) plate span ratio (plate length/bone fracture length), (4) number of empty holes (number of screw holes not inserted around the fracture), and (5) medial fracture distance (bone fracture distance on the medial side of the distal femur). Patient demographics (age), comorbidities (smoking, diabetes, chronic steroid use, dialysis), and injury characteristics (AO type, open fracture, infection) were obtained for all participants. Univariate analysis was performed on them. Results Of 71 fractures, 26 fractures were simple fractures, 45 fractures were comminuted fractures, and 7 fractures resulted in non-union. Non-union rate was significantly higher in comminuted fractures with bone medial fracture distance exceeding 5?mm. Non-union was founded in simple fractures with bone medial fracture distance exceeding 2?mm, but not significant (p Conclusions We concluded that bone fragment distance between fracture fragments is more important than bridge span length of the fracture site and the number of empty holes. Smoking and medial fracture distance are prognostic risk factors of nonunion in distal femoral fractures treated with LCP as bridging plate. Introduction Distal femoral fractures comprise only 0.4% of all fractures and 4–6% of femoral fractures [1, Regarding plate fixation, basic fixation is generally recommended to achieve absolute stability using lag screws in simple fractures; however, lag screw fixation cannot be performed in transverse fractures [7]. Moreover, it is impossible to achieve absolute stability with rigid internal fixation in comminuted fractures. In such cases, it is necessary to use a locking plate as a bridging plate to fix the fracture site [8]. The optimal insertion holes for the screws on the proximal side of the locking plate (when used as a bridge) are currently debated [9, Patients and methods This study received Institutional Review Board approval, and patients provided oral and written informed consents. The present study was approved by Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences and Okayama University Hospital (Ethics Committee No. 1712-035). This study included 71 distal femoral fractures in 70 patients (23 males, 47 females; mean age, 68.0?years [range, 16–91?years]) who were treated using the locking compression plate for distal femur (DePuy Synthes Co., Ltd, New Brunswick, CA, USA) at a university hospital and related facilities between April 2005 and December 2015. One female patient had bilateral femoral fractures. Cases in which the proximal and distal bone fragments were fixed using a lag screw and those in which the medial plate was used during the initial surgery were excluded. All surgery was performed by surgeons with more than 15?years of orthopedic experience at university hospital and related facilities. The mean follow-up period was 20.8?months (range, 5–33?months) (Table Table 1 Characteristics of distal femoral fractures Table 2 Characteristics of non-unions compared with fractures that healed In this study, we investigated (1) bone union rate, (2) bridge span length (distance between screws across the fracture), (3) plate span ratio (plate length/bone fracture length), (4) number of empty holes (number of screw holes not inserted around the fracture), and (5) medial fracture distance (bone fracture distance on the medial side of the distal femur). Bone union was defined as three out of four instances of cortical bridging on AP and lateral radiographs [12]. Non-union was defined as a state in which bone union was not achieved within 4?months after the initial surgery. Working length of a plate was defined as the distance between the first screws on either side of the fracture [13]. Plate span ratio was measured with reference to the length of the plate relative to the length of the fracture line, as proposed by Gautier et al. and Stoffel et al. [14, Fig. 1 HYPERLINK "https://josr-online.biomedcentral.com/articles/10.1186/s13018-019-1401-9/figures/1" Conclusive rules by Gautier et al. [14] and Stoffel et al. [15]. Fisher’s exact test was performed for statistical comparisons of open fractures, minimally invasive plate osteosynthesis, plate span ratio, and medial fracture distance between those with bone union (bone union group) and those with non-union (non-union group). The Mann-Whitney Results In this study, non-union was diagnosed in 7 of 71 cases. Non-union was diagnosed 2 of 26 (7.7%) cases with a simple fracture and 5 of 45 (11.1%) cases with a comminuted fracture (Table Table 3 Characteristics of simple fractures (OTA 33A2, C1) (n Table 4 Characteristics of comminuted fractures (OTA 33A3/C2/C3) (n The mean bridge span length of simple fractures in the bone union and non-union groups was 72.2?mm (range, 25–110?mm) and 72.5?mm (range, 45–100?mm), respectively (Table With respect to plate span ratio, 3 of 24 (12.5%) cases with simple fractures in the bone union group fit the plate length that was >?8–10 times longer than the overall fracture length, whereas 21 of 24 (87.5%) cases did not. Additionally, none of the cases in the non-union group fit the plate length of >?8–10 times longer than the overall fracture length (Table Of the cases with simple fractures, there was one non-union case with one empty hole and one non-union case with four empty holes (Table Of 26 simple fractures, there were 7 cases with a medial fracture distance of ≥?2?mm, and the non-union rate was 28.5% (2 of the 7 cases) (Table Open fractures were observed in 19 of 71 (26.8%) cases (Table Several example cases are shown in Figs. Fig. 2
a Fig. 3
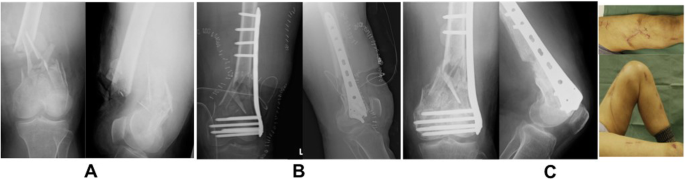
a Fig. 4
a In case 3, it showed that plate length was 196?mm, fracture distance was 65?mm, plate span ratio was 196/65 = 3.01, bridge span length was 85?mm, medial fracture distance was 0?mm (because of shortening fracture site), and empty hole number was 1. Performing shortening and fixation of up to 5–10?mm was effective for achieving bone union in several comminuted fracture cases (Fig. Discussion During surgery, it is sometimes difficult to properly determine screw position. Thus, the purpose of this study was to examine the appropriate screw position in relative fixation. The guidelines reported by Gautier et al. suggested that a locking compression plate should be used as a bridging plate in order to achieve relative stability. Additionally, the researchers recommended that the plate length used in simple fractures should be 8–10 times longer than the fracture length, 0–3 empty holes should be left in the surrounding space, the distance space should be ≤?2?mm, and ≥?3 screws should be inserted (bicortically) into the proximal and distal bone fragments [14]. For comminuted fractures, the guidelines recommend that the plate length should be at least 2–3 times longer than the fracture length and ≥?3 empty holes should be left in the surrounding fracture site. Additionally, according to Stoffel et al., the number of empty holes, including the fracture site, should be between one and four in simple fractures, and in comminuted fractures, the screws should be inserted as close to the fracture site as possible [15]. Although screw insertions near the fracture site increases fracture stability, in some cases, this may result in a lack of proper fracture micro-motion, leading to poor callus formation [17]. The “far cortical locking technology” was demonstrated to increase fracture stability and flexibility; however, long-term results have not yet been obtained [18]. Megas et al. reported that fracture site instability prevents bone callus formation, even with good blood supply [19]. In most of our cases, non-union likely resulted from fracture site instability after reduction internal fixation. Henderson et al. reported no plate length differences between non-union and union groups, which was similar to our results [20]. Elkins reported favorable callus formation with a bridge span length of ≤?80?mm. Conversely, fracture instability was significantly higher with >?80?mm of bridge span length, which resulted in poor callus formation [21]. Lujan et al. reported that callus formation decreases as the bridge span length increases [22]. Bottland et al. reported that increasing fracture site flexibility promotes initial bone formation, but had no correlation with bridge span length [23]. Additionally, Henderson et al. reported no significant differences in bridge span lengths of 64.4 and 69.8?mm in two respective cases of non-union and union [20]. Our study also showed no significant differences between groups (Tables Stoffel et al. advised to reduce the fracture site distance to ≤?2?mm [15]. In our study, 7 of 26 simple fracture cases had a medial fracture distance of ≥?2?mm, and non-union was observed in 2 of these 7 (28.5%) cases. Additionally, of the 45 cases with comminuted fractures, 13 cases had a medial fracture distance of ≥?2?mm, and non-union was observed in 4 of these 13 (30.7%) cases. Bone union was observed in all cases with simple or comminuted fractures with respective medial fracture distances of ≤?2?mm or ≤?5?mm. Based on our findings, we concluded that bone fragment distance between fracture fragments is more important than bridge span length of the fracture site and the number of empty holes. Reducing comminuted bone fragments is difficult when the inner portion of the fracture site also exhibits comminuted fracture. In such cases, shortening the fracture site to approximately 5–10?mm would be acceptable to decrease the distance between the proximal and distal bone fragments. Regarding the number of empty holes, Stoffel et al. recommended opening 1–2 holes close to the fracture sites in simple fractures and inserting the screws as close as possible to the fracture sites in comminuted fractures [13]. In Henderson et al.’s study involving 70 patients, the average number of empty holes proximal to the fracture site was 0.3 in the non-union group and 1.1 in the bone union group [20]. Additionally, Bottlang et al. observed a 19% bone union failure rate in a cohort of 70 patients and reported that there were significantly more empty holes proximal to the fracture site in the patients with non-union compared to those with successful bone union [23]. In our study, while there were no clear differences in the non-union rates as a result of the number of empty holes, non-union rate tended to increase as the number of empty holes increased in the proximal fragment in some cases. We believe that by decreasing the number of empty holes around the fracture site (i.e., inserting the screw near the fracture site), fracture site stability increased. Even with relative fixation, the more the empty hole, the higher the risk of a non-union, because bone union was achieved during salvage surgery in non-union cases through plate replacement with a long plate or inserting a screw near the fracture site. Risk factors for non-union and delayed bone union in distal femoral fractures include the presence of open fracture(s), medial bone defects, and comminuted fracture(s) [3, Table 5 Healing complications of distal femoral fractures treated with locking plates Study limitations included its retrospective design and the relatively small sample size. A senior medical doctor with >?15?years of experience as an orthopedic surgeon operated on these cases; therefore, a certain surgery quality (reduction of fractures, treatment of soft tissues) was guaranteed. We analyzed several independent variables to determine how they impacted fracture healing; however, it is possible that other variables that were not considered may have contributed to the outcomes. Additionally, although we did not consider bone mineral densities and BMI, there is a possibility that they might have influenced bone union. Conclusions In distal femoral fractures, non-union sometimes may occur, despite improvements in implant and reduction techniques. Well-known risk factors include smoking, bone defects, and comminuted fractures, which were supported by this study’s results. The bone fracture distance on the medial side of the distal femur was related to bone union rather than screw position. These results will be helpful in treating distal femoral fractures with plates. Based on our findings, we concluded that bone fragment distance between fracture fragments is more important than bridge span length of the fracture site and the number of empty holes. The number of empty holes near the fracture site and the rate of bone healing were not clearly related. Availability of data and materials The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. Abbreviations AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association AP: Antero-posterior LCP-DF: Locking compression plate for distal femur References 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 PubMed 19 20 21 22 23 24 25 26 27 28 29 30 31
|

Shanghai Carefix Medical Instrument Co., Ltd.China
滬ICP備16042301號-1 (滬)-非經(jīng)營性-2016-0122 滬食藥監(jiān)械生產(chǎn)許20101725號
