|
News Detail
One-Stage Closed Intramedullary Nailing for Delayed Femoral Fracture in Multiple Injured Patients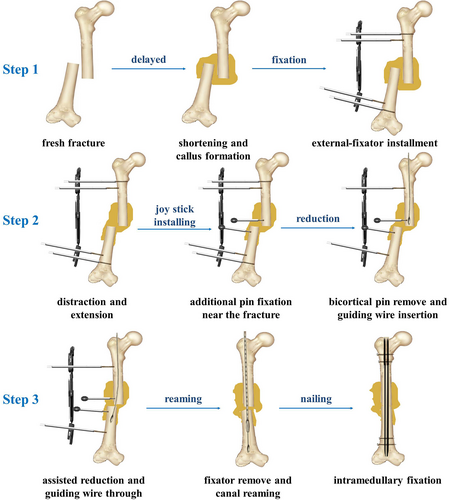 Introduction The delayed femoral fracture with limb shortening and callus formation is still difficult to handle even for the most experienced clinicians. It is an uncommon circumstance when the fracture is not managed in a timely manner in cases of life-threatening polytrauma. Closed intramedullary nailing is the gold standard treatment for acute femoral fracture with good clinical outcomes in adults. However, the operation of the delayed fracture is usually fraught with complications due to failed reduction and the rehabilitation process is often tedious. Nowadays, open reduction for the delayed femoral fracture is often carried out to treat such fractures, but their clinical outcomes are less satisfactory as compared to the cases of fresh femoral fractures7. A preoperative traction or staged surgery is thought necessary for the cases with obvious gross overriding to avoid neurovascular complications associated with acute lengthening more than 4 cm. However, the duration of such treatments is prolonged significantly with less compliance of the patient and potential infection risk. A previous study demonstrated that open reduction is often necessary in patients with fractures delayed for more than 8?weeks. In another study, a second-stage open tissue release and fracture reduction were adopted for intramedullary nailing after preoperative skeletal traction, but bone grafting was needed, which increased surgery complication and medical cost greatly. A recent study reported that a single-stage open nailing technique using judicious bone resection and manual traction could be applied intraoperatively without preoperative skeletal traction. However, this open reduction and fixation resulted in more tissue injury and blood loss with higher potential infection risk. Actually, the main obstacle for closed intramedullary nailing is the laborious reduction of the fracture intraoperatively because of the limited strength of the local distractor or traction table. Minimally invasive nailing with closed reduction might be an ideal solution to achieve fracture union and minimize iatrogenic interference. Clinically, the unilateral extendable external fixator can produce enough extension power in resisting axial compression or extension. Nowadays, the external-fixator system is generally used in distraction osteogenesis and fracture reduction in lower extremity with satisfactory clinical outcomes. Hence, we proposed to use the unilateral external fixator to provide strong mechanical strength to distract the fracture ends for closed reduction in delayed femoral fracture. To the best of our knowledge, the one-stage closed intramedullary nailing has not been explored for delayed femoral fracture so far. The present study aims to investigate: (i) whether the closed reduction can be acquired by the unilateral extendable external fixator in delayed femoral fracture; (ii) whether the one-stage closed intramedullary nailing can be carried out effectively for patients; (iii) the clinical effects and functional recovery of this technique. We hypothesized that our strategy could provide a minimally invasive treatment for the patients with delayed femoral fracture and have good clinical outcomes. Methods Inclusion and Exclusion Criteria A retrospective study was carried out on delayed femoral shaft fracture treated by the fixator-assisted nailing technique between February 2008 and January 2017. The institutional review board of our hospital approved the study and informed consent was obtained from each patient. The inclusion criteria were as follows: (i) patients aged 18 to 60?years with delayed femoral fracture; (ii) the fracture was treated by the one-stage internal fixation technique; (iii) observation and check were followed for more than 1?year with detailed outcome records for all the patients. The exclusion criteria were as follows: (i) pathological fracture due to organic lesions (e.g. tumor, tuberculosis, and infection); (ii) local infection around the fracture; (iii) malunited fractures. Surgery Process Preoperative Evaluation The brief diagram of this technique is shown in Fig.
Fig. 1 Open in figure viewerPowerPoint Diagram of the minimally invasive fixator-assisted nailing technique for the delayed femoral shaft fracture. Anesthesia and Position Careful evaluation of the skin and soft tissue at the surgical site was also carried out in accordance with the basic surgical protocol. Antibiotics were delivered 30 min prior to the surgery in order to prevent infection. The general anesthesia was applied and the patient was placed on a traction table in supine scissor position, keeping feet neutral with boot traction. Thereafter, a routine disinfection and draping procedure was conducted. Approach and Exposure For the reduction of the shortened fracture, an standard Orthofix unilateral extendable external fixator (Procallus 90,001, OrthofixOrthopaedic External Fixator Systems, OrthofixSrl, Fracture Reduction For the convenience of reduction procedures and fluoroscopy observation, the external fixator was fixed on the anterior-lateral plane of the thigh. The affected limb was distracted on the traction table until the joint space of hip was obviously widened in C-arm fluoroscopy (SIREMOBIL Compact L, Siemens, Shanghai, China). Subsequently, the adjustable turnbuckle on the external fixator was extended gradually to distract the overlapping fracture ends. After application of the above steps alternatively, the shortened fracture was overdistracted moderately for the subsequent reduction. This overdistraction was maintained by the fixator for about 5–10 min to loosen the contracted soft tissue. Thereafter, bicortical pins were screwed in and the limb length was maintained by both the traction table and the external fixator with an unicortical pin on each side. An additional unicortical pin with clamp was screwed into the femoral shaft on each side near the fracture ends as a joy stick to facilitate the closed reduction and insertion of the guide wire thereafter. Intramedullary Nailing and
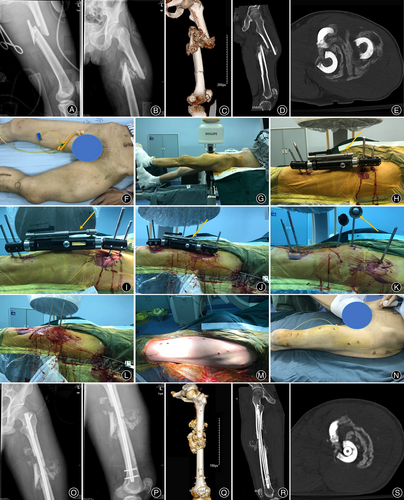
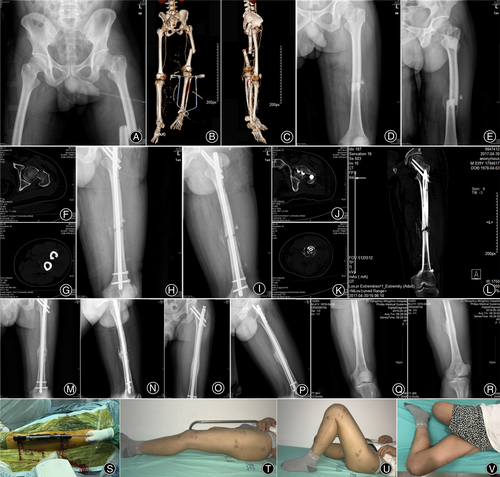
Fig. 2 Open in figure viewerPowerPoint A representative case with fracture type 32B2 (38?days, 79?mm) was treated by the fixator-assisted nailing technique at one stage. (A) Initial fresh femoral shaft fracture after injury. (B) Delayed femoral shaft fracture with callus formation. (C, D, E) CT scan showed massive callus surrounding the fracture ends and obvious limb shortening. (F) Gross view of the deformity and callus lump. (G) The patient was placed on a traction table in supine scissor position, keeping feet neutral with boot traction. (H) An extendable external fixator with an adjustable turnbuckle was implemented over the fracture. (I) The fracture was moderately overdistracted by the external fixator to release the soft contracture and restore the length of the femur. (J) Two additional unicortical pins were fixed on the shaft as joy sticks near the ends of the fracture. (K) The joy sticks were used to assist insertion of the guide wire into distal medullary cavity. (L) The end of guide wire was centered in the distal femur and confirmed by the fluoroscopy. (M) After removing the external fixator and all pins, the intramedullary nail was inserted and fixed. (N) Incisions for this technique are minimally invasive. Postoperative radiographic evaluation in (O) AP view and (P) lateral view. (Q, R, S) CT scan showed the fracture reduction and nail fixation. The shortening deformity had been corrected and the callus remained around the fracture site.
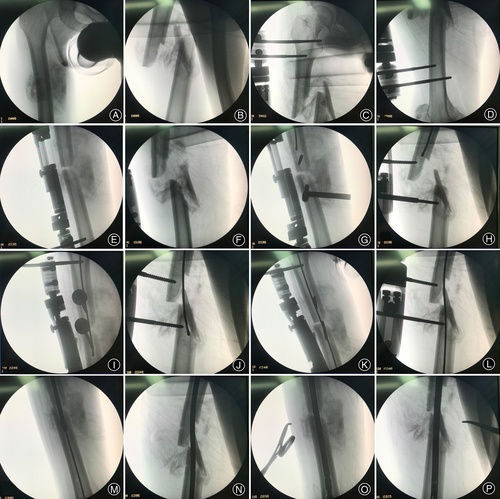
Fig. 3 Open in figure viewerPowerPoint Intraoperative images for the illustration of the fixator-assisted nailing technique. (A-B) Preoperative fluoroscopy showed obvious shortening deformity of the fracture and massive callus around. Two pins were fixed on the proximal (C) and distal (D) fragment part of the fracture. The space of hip was obviously widened due to the skin distraction on the limb (C). (E-F) The overlap of the fracture was extended to moderate overdistraction on fluoroscopy by the external fixator. (G-H) Additional pins were screwed in as joy sticks and the guide wire arrived at the proximal fracture end. (I-J) With the assistance of the external fixator and joy sticks, the guide wire was successfully passed through the fracture site (K-L) The guide wire was inserted into the distal medullary cavity. (M-N) The reamer was applied to expand the medullary cavity over guide wire. (O-P) The nail was inserted into the femoral canal to reduce and fix the fracture. Postoperative Rehabilitation On the second day after operation, the patients were instructed to perform passive functional exercise of the operated limb. Weight bearing was dictated by the stability of the fracture and the associated injuries. The patients who were capable of out-of-bed activity were encouraged to gradually implement weight-bearing exercise 1?week after the operation. When radiographic union was seen, the patient was encouraged to full-weight bearing. The patients were visited and their recovery statuses were checked routinely thereafter at least for 12 Clinical Indicators Fracture Union Quality of the fracture reduction and fixation was assessed by postoperative radiographs. The limb length discrepancy and rotation deformity in the patients were evaluated by computed tomography scanning. The postoperative evaluation of the fracture union was performed with the help of radiographs. Union was defined as the nontender fracture site in a patient who was able to bear full weight and had continuous bridging callus on anteroposterior and lateral radiographs. The diagnosis of non-union was made in the presence of abnormal movement at the fracture site at least 9?months after the injury and with no progressive signs of healing for at least 3?months, despite continuous treatment. Whereas malunion was defined as shortening of more than 2.5 cm and angular deformity of more than 10°. Visual Analog Score (VAS) The VAS score system used in the social and behavioral sciences was adopted to measure lower limb pain. The VAS pain scoring standard (scores from 0 to 10) is as follows: 0 means painless; 1–3 means mild pain that the patient could endure; 4–6 means that patient is in pain that could be endured, but the patient is unable to sleep; and 7–10 means that patient has intense pain and is unable to tolerate the pain. Knee Mobility Postoperative management with regard to weight-bearing and the range of motion of the extremity was individualized according to the fracture stability and associated injuries. Functional outcomes were assessed postoperatively mainly based on knee flexion and extension with a goniometer by a senior author. Statistical Analysis The SPSS (version 18.0, SPSS Inc. Chicago, Illinois, USA) was applied to analyze the data obtained from our study. The measurement data such as BMI, injury severity scores, time to nailing, callus-to-diaphysis ratio, surgical time, follow-up duration, fracture-union time, length of hospital stay, and VAS were described as a value of mean?±?SD (standard deviation). The age was recorded as median, minimum, and maximum value. The gender, afflicted side, injury mechanism, fracture type, and reduction method were described as categorical data. Comparison of angle deformity, rotational deformity, and limb shortening distance was performed by paired t-test with a statistical significance level set at Results General Results A total of 13 patients (16 sides) who underwent fixator-assisted nailing surgery were registered for the study, including 10 males and three males with a median age of 39?years. Among them, 11 patients (14 sides) were successfully treated by the one-stage closed intramedullary nailing, while two patients (two sides) failed and had to be converted to open internal fixation. There were five patients with fracture on the right side, five patients on the left side, and three patients on both sides. Demographics and details of the patients are summarized in Table TABLE 1.
* Previously, eight patients were treated with cast or brace immobilization in basic medical institutions. When the patients were referred to our center, the femoral fracture was delayed. While the other five patients were managed by skeletal traction in the intensive unit of our hospital due to the severe multiple injuries, the length of the femoral shaft was not maintained well. The average duration of the time-after-fracture was 38?days, with the longest one reaching 110?days. All the patients had other system or skeletal injuries, that affected the management and outcome of the femur fracture. Thirteen patients had at least another long bone and craniocerebral or chest injuries besides the femoral fracture. There were four open fractures based on the Gustilo–Anderson classification system. The mean injury severity score (ISS) of the patients was 32.77?±?9.98 (range 19 to 52). According to the AO/ASIF classification, among the patients, there were two 32A1 type fractures, six 32A3 type fractures, four 32B1 type fractures, two 32B2 type fractures, one 32B3 and one 32C3.3 type fractures, respectively, including a concomitant ipsilateral femoral neck fracture and trochanteric fracture. Intraoperative Records The unilateral femoral fracture was carried out for the patients. The average operation time of unilateral femoral fracture was 192.19?±?29.38 min, with the longest time of 270 min. The average intraoperative blood loss was 587.50?±?232.02 ml, ranging from 300 to 1200 ml. In one case, the closed reduction on the left side failed, so open reduction was resumed for the operation which led to additional blood loss and long operation time. As the patient could not withstand another operation, the right side was successfully treated by closed reduction using the fixator-assisted nailing technique 1?week later. Clinical Outcomes Fracture Union The discrepancy of lower limb was recovered from preoperative 35.48?±?19.24?mm to post operation 3.87?±?2.52?mm. The rotation deformity of femur was corrected from preoperative 30.39°?±?13.99° to post operation 5.09°?±?2.70°. All the patients had an effective fixation and restoration of limb alignment. There was limb discrepancy of more than 5?mm in three patients, which could be managed by height correction footwear. All the patients were followed up successfully with an average time of 21.62?±?4.99 Visual Analog Score (VAS) For all the patients who had the operation, there were no major complications such as infection, compartment syndrome, neurologic, or vascular complications. The mean VAS score was 1.63?±?1.09 at the final follow-up. There were four non-specific painful thighs in the first 3?months, which would be relieved by oral analgesic drug. Knee Mobility The mean maximal knee flexion was 131.25?±?5.32 degree at the final follow-up. A mild decrease in the range of motion of the knee occurred in three patients. All the patients were satisfied with their improvement in movement, and the operation did not affect their work and daily activities. Detailed clinical outcomes of the patients were summarized in Table TABLE 2.
*
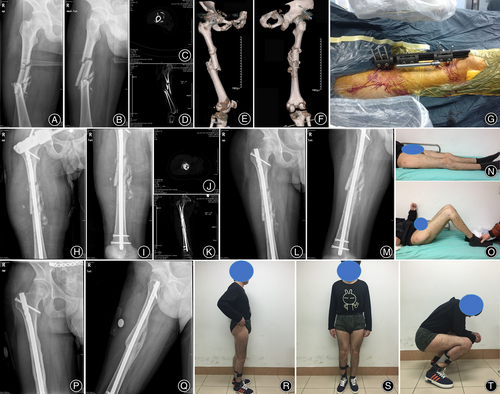
Fig. 4 Open in figure viewerPowerPoint A representative case, which had a femoral shaft (32B2 type) and concomitant neck fracture, was delayed for 36?days with 20-mm shortening by the external-fixator assisted intramedullary nailing technique. (A) The radiograph at injury time showed fresh femoral shaft fracture with obvious displacement. (B-C) The 3D images showed shortening and angular deformity both in AP view and lateral view. The other side limb was amputated due to severe trauma in an accident before. (D-E) Twenty-four days after initial trauma, the preoperative radiographs showed the delayed femoral shaft fracture with callus formation and shortening. (F, G) CT scan indicated the overlapping and displacement of the fracture, and the concomitant femoral neck fracture was on the same side. (H-I) Postoperative radiographs showed good reduction and effective fixation of the fracture. (J, K, L) CT scan indicated the femoral shaft and neck fracture were fixed effectively with good reduction and fine alignment. The shortening and displacement of the fracture had been corrected with intramedullary nailing. (M-N) The radiographs at 3-months postoperatively showed fracture union. (O-P) On the final radiographs obtained at 22
Fig. 5 Open in figure viewerPowerPoint A 32C3.3 type fracture which was delayed for 38?days with 23.26?mm overlapping. (A-B) Overlapping and varus angulation were seen at the fracture site with callus formation. (C, D, E, F) CT indicated obvious shortening and displacement of the fracture with massive callus surrounding the fracture site. (G) The external fixator was applied to assist the fracture reduction and nail fixation. (H-I) Postoperative radiographs showed restoration of the alignment and effective fixation of the fracture. (J, K) The shortening and displacement of the fracture had been corrected with intramedullary nailing fine alignment of the femoral shaft. (L-M) Follow-up radiographs after 2.8?months from surgery showed fracture union with partially restricted knee function (N, O). (P-Q) On the final radiographs obtained at 24 Discussions Delayed femoral fracture, due to lack of effective traction, reduction, or immobilization, is still a problem in developing and underdeveloped nations. It is invariably associated with shortening and tissue contracture. Its treatment seems not to be addressed sufficiently considering the paucity of literature. Our results showed that: (i) the unilateral extendable external fixator could provide sufficient mechanical distraction strength for the shortened delayed femoral fractures; (ii) the fixator-assisted nailing technique could achieve good closed reduction for most cases; (iii) the one-stage protocol could promote the fracture union and have low complication rate with satisfactory functional recovery. Effectiveness of the Fixator-Assisted Intramedullary Nailing Clinically, closed reduction and nailing fixation are effective for stable hip fracture with good clinical results. In distal femur shaft fractures, both retrograde nailing and locking plate could provide good subjective and objective results. As for nonunions and malunions of distal femoral fracture, the bio-metallic solution could recreate the knee anatomy and functionality with satisfactory quality of life. However, breakage of the nail and high non-union rate were occasionally observed due to insufficient reduction in unstable subtrochanteric fractures. Under such circumstances, the combination of the lateral blade plate and the medial bone splint might be a definitive technique for bone union. As for multi-fragmentary segmental femoral shaft fractures, the open reduction and plate fixation with bone strut allograft had better clinical results compared to the minimally invasive plate osteosynthesis technique. Actually, stability of the unstable femoral fractures mainly relies on good reduction, including slight valgus alignment and positive medial cortical support in displacement, and central axial alignment with smooth anterior cortex contact. However, the optimal treatment of delayed femoral fractures has not been well-acknowledged and documented so far. As for the delayed fracture, the shortening limb is difficult to be distracted by tract table or bone distractor intraoperatively. Meanwhile, the callus and scar tissue can hinder reduction of the fracture, and open reduction has been adopted to tackle this obstacle by some physicians. In a previous study, a mean length of 9-mm bone resection was carried out to achieve reduction in nine of 14 patients, which were treated by the single-stage open intramedullary nailing. Another study showed good results in patients with a similar technique, however, five of the 17 patients required a blood transfusion either intraoperatively or postoperatively, and the mean fracture union time was 16?weeks. In another series of 11 patients with isolated femoral fractures treated by open nailing, preoperative traction was used in five cases with one patient required a bone resection. Although 10 patients had femoral fracture union at a mean time of 11.9?weeks, eight of the 11 patients had to undergo iliac crest bone grafting operation. In our study, all the patients acquired fracture union, and the mean fracture union time was 12?weeks with no bone grafting. The closed reduction protected the blood supply and extra-periosteal tissues well, so that it could facilitate the fracture healing effectively. Meanwhile, the process of reaming established freshness of the broken ends of the fracture and was associated with re-canalization of the medullary cavity which is beneficial to fracture healing. Furthermore, the original callus Tolerance of Acute Lengthening in Femoral Fracture Previous studies have shown that acute lengthening would not affect knee movement significantly and it is safe for a lengthening up to 4 cm. In the present study, the maximal lengthening distance was 79?mm with no vascular or nerve complications. The main reason for such long distraction might be the elastic potential of the soft tissue with the limited duration of the shortening of the fracture. However, too large acute lengthening will cause an increased risk of neurovascular injury. In this series, the patients had equal limb lengths before the trauma that led to the shortening which resulted from the initial injury. The neurovascular structures were initially of normal length. Furthermore, the femoral shaft is surrounded by larger, less-compact musculotendinous compartments and therefore its soft tissue envelope had more potential for the lengthening. The femoral non-unions, unlike malunions, are mobile, have less adherent, contracted, and resistant scar tissue, and appear to tolerate more lengthening without the risk of neurovascular compromise as was reported with lengthening of malunited femora. Previous research demonstrated that as much as 5 cm of acute lengthening of a shortened femur with non-union is possible, with a low prevalence of neurovascular compromise. Some Tips for the Closed Reduction of Fracture In this study, we used the standard Orthofix unilateral extended external fixator system to distract the shortened fracture ends for the closed reduction. Due to the large pin diameter (6?mm) and strong fixator frame, this system has better mechanical strength than the bone distractor. Generally, the Orthofix external fixator has been widely applied in open fracture and limb lengthening in lower extremities with satisfactory clinical outcomes. For the successful closed reduction of the delayed femoral shaft fracture, the following tips should be kept in mind: (i) the affected limb should be distracted by the tract table until widening of the hip joint before implementation of the fixator; (ii) the distraction of the extendable external fixator and tract table should be carried out alternatively to restore the femoral length; (iii) the fracture site should be over-distracted moderately for convenience in the reduction; (iv) the pin should be screwed into the bone cortex unilaterally to allow it passing through the guide wire into the canal; (v) after the insertion of the guide wire into the distal part, the centralization of the wire is important for the minimization of the angular deformity. Traditionally, denser-looking callus indicates a stiffer healing region based on human subjective interpretation of the quality and quantity of visible callus in radiographic view. A previous study showed that the callus volume and density do not correlate with the structural integrity of the partially healed bone qualitatively. We found that the fracture displacement with one plane back-to-back override was the most appropriate technique for this patient. The interface between the callus and femoral shaft might predict the connectivity of the healing zone more accurately. In the present study, the alignment of the fracture and limb length was recovered satisfactorily for all cases. Limits of the Study There are still some limits in the present study. First, the number of our cases was small and the study span was long, because the delayed femoral shaft fracture is not common. Second, it could be improved by comparing our cases with patients who have been treated by the staged or open intramedullary nailing. Third, by using both Orthofix external fixator and intramedullary nailing, the cost is increased significantly by this technique and should give full consent to the patient. Fourth, the time spans of our cases are long, there are some other factors that might bias the results in this retrospective study. Conclusion Although delayed femoral facture is uncommon, they should be addressed with more attention due to the morbidity caused; this is especially important for underdeveloped countries. Our attempt to treat delayed femoral shaft fractures with closed intramedullary nailing have shown facilitated fracture union, low complication rate, and early recovery of the functions. The one-stage fixator-assisted nailing provides a minimally invasive strategy for most of the patients safely and restores the extremity length, thus it is a useful and effective technique. Acknowledgments This work was supported by the National Key R&D program of China (2018YFA0701401), the Key R&D program of Zhejiang Province (2021C03108, 2021C04G2013057), Joint Construction Project of Zhejiang Province and Health Ministry (WKJ-ZJ-2029), Zhejiang Natural Science Foundation (Y22H069063), Foundation of Zhejiang Educational Committee (Y202147225). It was an outcome of a continuing partnership among all authors. The authors would like to acknowledge the staff of Orthopaedic Lab of Zhejiang University for their assistance. None of the authors had professional or financial affiliations that biased this work. Author Contributions Ruijian Yan: collection and assembly of data; data analysis and interpretation; manuscript writing. Yifan Wu: collection and analysis of data; data interpretation, manuscript writing. Yiying Qi: collection of data; data analysis and interpretation. Hang Li: data analysis and interpretation. Shurong Dong: conception and design; data analysis and interpretation; final approval of manuscript. Feng Gang: conception and design; data analysis and interpretation; revision of the manuscript, financial support, group leader.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

Shanghai Carefix Medical Instrument Co., Ltd.China
滬ICP備16042301號(hào)-1 (滬)-非經(jīng)營(yíng)性-2016-0122 滬食藥監(jiān)械生產(chǎn)許20101725號(hào)
